We have previously commented on the many scientific mistakes in the WHO draft Monograph on radiofrequency fields and health effects. Since there has not been any reaction we have sent the following letter asking for revision. A similar letter was send to IARC asking for new cancer risk evaluation.
World Health Organization 4 August, 2015
Dr Margaret Chan, Director General
World Health Organization
Avenue Appia 20, 1211 Geneva 27
Geneva, Switzerland
Emelie van Deventer, Team Leader
Radiation Programme Department of Public Health,
Environmental and Social Determinants of Health,
World Health Organization
Geneva, Switzerland
Dear Ms. Margaret Chan
Dear Ms. Emelie van Deventer
Further Comments on the WHO draft: Radio Frequency fields: Environmental Health Criteria Monograph
On 15 December, 2014 we submitted comments on the WHO draft on radio frequency fields and health. Since we have not got a satisfactory reply from WHO, not seen a revision of the draft, and adding to that more published studies that reinforce the increased risk for certain brain tumours associated with use of wireless phones we want to submit the following, additional comments.
The brain is the primary target organ for exposure to radiofrequency electromagnetic fields (RF-EMF) during the use of the handheld wireless phone. This has given concern of an increased risk for brain tumours. The carcinogenic effect of RF-EMF on humans was evaluated at a meeting during 24 – 31 May 2011 at the International Agency for Research on Cancer (IARC) at WHO in Lyon, France. One of us (LH) was part of the expert group. The Working Group categorised RF-EMF from mobile phones, and from other devices that emit similar non-ionising electromagnetic fields in the frequency range 30 kHz–300 GHz, as a Group 2B, i.e. a possible, human carcinogen (http://monographs.iarc.fr/ENG/Monographs/vol102/mono102.pdf).
Since then more studies have been published that strengthen the association between use of wireless phones (mobile and cordless phones) and increased risk for brain tumours. We have performed long-term research in this area and in the following we give a short up-dated summary of our findings based on research since the 1990’s. In our publications relevant information can be found also on other studies, as well as discussions of the current scientific evidence.
Glioma:
Glioma is a malignant brain tumour (“brain cancer”), and the most common type is glioblastoma multiforme with a poor prognosis. We have published a statistically significant increased risk for glioma among users of both mobile and cordless phones. The risk increased with latency (time from first use of the phone until tumour diagnosis) and cumulative number of hours for use. Highest risk was found in the area of the brain with highest exposure to RF-EMF. All these results are of biological relevance; that is what would be expected for a causal association. The full paper can be read here:
http://www.pathophysiologyjournal.com/article/S0928-4680(14)00064-9/pdf
Meningioma:
Menigioma is mostly a benign brain tumour and accounts for about 30 % of all intracranial tumours. The incidence is approximately 2-times higher in women than in men. No conclusive evidence of an association between use of mobile and cordless phones and meningioma was found in our study. However, taking the long latency periods that have been reported for the increased meningioma risk associated with exposure to ionizing radiation it is still too early to make a definitive risk assessment. Results for even longer latency periods of wireless phone use than in our study are desirable, see more details here:
http://www.spandidos-publications.com/or/33/6/3093
Acoustic neuroma:
Acoustic neuroma or Vestibular Schwannoma is a rare benign tumour in the eighth cranial nerve that leads from the inner ear to the brain. It grows slowly and does not undergo malignant transformation, but may give compression of vital brain stem centres. Tinnitus and hearing problems are usual first symptoms of acoustic neuroma. We published a clear, statistically significant, association between use of mobile and cordless phones and acoustic neuroma. The risk increased with time since first use. For use of both mobile and cordless phones the risk was highest in the longest latency group. Tumour volume increased per 100 hours of cumulative use and year of latency for wireless phones indicating tumour progression from RF-EMF. The whole study can be read here:
http://www.spandidos-publications.com/ijo/43/4/1036
Brain tumour prognosis:
A causal association would be strengthened if use of wireless phones has an impact on the survival of glioma patients. We analyzed survival of 1,678 glioma patients in our case-control studies 1997-2003 and 2007-2009. Use of wireless phones in the > 20 years latency group (time since first use) yielded increased hazard ratio (HR) = 1.7, 95 % confidence interval (CI) = 1.2-2.3 for glioma, i.e. decreased survival. Increased HR was found for use of both mobile and cordless phones. Highest HR was found for cases with first use before the age of 20 years. These results strengthen a causal association between use of wireless phones and glioma. The publication can be read here:
http://www.mdpi.com/1660-4601/11/10/10790
Risk in different age groups of first use:
In our glioma study we found highest risk for subjects with first use of mobile or cordless phone before the age of 20, see Table 8 in the publication:
http://www.pathophysiologyjournal.com/article/S0928-4680(14)00064-9/pdf
We published similar results for acoustic neuroma and use of mobile phones, see Table 21.2:
http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.433.7480&rep=rep1&type=pdf
Children and adolescents are more exposed to RF-EMF than adults due to thinner skull bone, higher conductivity in the brain tissue, and a smaller head. The developing brain is also more vulnerable than in adults and it is still developing until about 20 years of age. The finding of higher risk in young persons is worrying, not the least due to the high prevalence of use of wireless phones in children and adolescents.
Brain tumour incidence:
It is not correct to claim that the incidence of brain tumours has not increased in the Scandinavian countries. The age-standardized incidence of brain tumours increased dramatically in Denmark with +41.2 % among men and +46.1 % among women during 2003-2012 (http://www.ssi.dk/Aktuelt/Nyheder/2013/~/media/Indhold/DK – dansk/Sundhedsdata og it/NSF/Registre/Cancerregisteret/Cancerregisteret 2012.ashx).
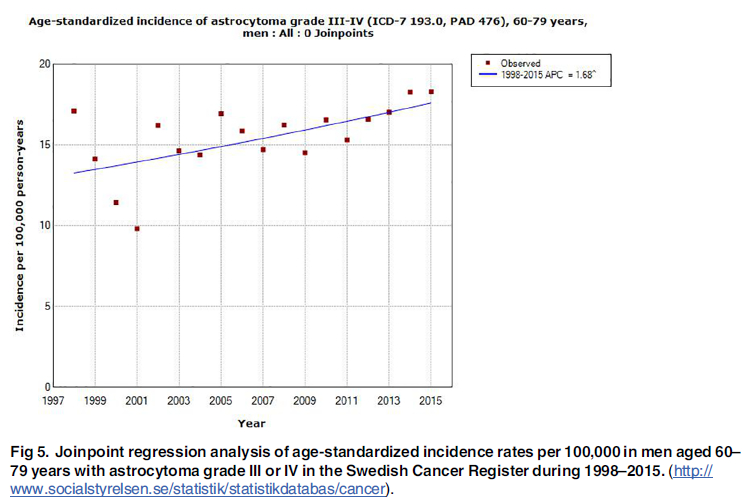
Due to the well-known under-reporting of brain tumours to the Swedish Cancer Registry we studied brain tumour rates using the Swedish National Inpatient Register and the Causes of Death Register (see http://www.mdpi.com/1660-4601/12/4/3793/htm ). In summary we found a statistically significant increasing rate of not specified brain tumours from 2007 in the Inpatient Register and from 2008 in the Causes of Death Register. Our study indicated that several of these tumours were never reported to the Swedish Cancer Register. The results are in accordance with a reasonable latency period for use of wireless phones, e.g. mobile phones, see Figures 5 and 6 in our publication. Thus, the Swedish Cancer Register data cannot be used to dismiss an increased risk for brain tumours associated with use of wireless phones. On the contrary our study is consistent with an association considering a reasonable tumour induction period.
Mechanistic aspects:
– Reactive oxygen species:
RF-EMFs do not cause direct DNA damage. On the other hand numerous studies have shown generation of reactive oxygen species (ROS) that can cause oxidative damage of DNA. This is a well-known mechanism in carcinogenesis for many agents. The broad biological potential of ROS and other free radicals makes radiofrequency radiation a potentially hazardous factor for human health, not only cancer risk but also other health effects. A recent update can be read here:
http://informahealthcare.com/doi/abs/10.3109/15368378.2015.1043557
-Tumour promotion:
Tumour promotion by RF-EMF exposure was reported in 2010 in a study on mice: http://www.ncbi.nlm.nih.gov/pubmed/20545575. These findings were recently replicated and add to the relevance of tumour risk: http://www.ncbi.nlm.nih.gov/pubmed/25749340
-p53:
The p53 protein is a transcription factor that plays a vital role in regulating cell growth, DNA repair and apoptosis, and p53 mutations are involved in disease progression. In a recent study it was found that use of mobile phones for ≥3 hours a day was associated with increased risk for the mutant type of p53 gene expression in the peripheral zone of astrocytoma grade IV (glioblastoma multiforme), and that this increase was statistically significant correlated with shorter overall survival time:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4178273/
These results are in agreement with the decreased survival for patients with astrocytoma grade IV (glioblastoma multiforme) associated with long-term use of mobile phones and cordless phones that we reported in 2014, see above the section on prognosis.
Causality:
To further evaluate strengths of evidence Sir Austin Bradford Hill wrote in the 1960’s a famous article on association or causation at the height of the tobacco and lung cancer controversy: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1898525/pdf/procrsmed00196-0010.pdf
Hill offered a list of nine aspects of an association to be considered when deciding if an association is causal. However, he did not request all nine viewpoints to be fulfilled for causality. We used the Hill criteria to evaluate the causality on brain tumour risk from RF-EMF emitted from wireless phones. We concluded that based on the Hill criteria, glioma and acoustic neuroma should be considered to be caused by RF-EMF emissions from wireless phones and regarded as carcinogenic to humans, classifying it as Group 1 according to the IARC classification. See more here:
http://www.degruyter.com/view/j/reveh.2013.28.issue-2-3/reveh-2013-0006/reveh-2013-0006.xml
Conclusion:
Our results are in agreement with other studies such as the international Interphone study and the French CERENAT study. This is discussed in more detail in e.g. our article on glioma risk, see also:
http://www.pathophysiologyjournal.com/article/S0928-4680(12)00110-1/pdf
The so called Danish cohort study on mobile phone users has been taken as evidence of no risk. However, the many shortcomings as reviewed elsewhere makes the study inconclusive regarding assessment of cancer risk. It should not be cited as evidence of no risk, for more details see: http://www.degruyter.com/view/j/reveh.2012.27.issue-1/reveh-2012-0004/reveh-2012-0004.xml?format=INT
In summary there is consistent evidence of increased risk for glioma and acoustic neuroma associated with use of mobile phones and cordless phones. Furthermore, the risk is highest for persons with first use before the age of 20, which is of special concern. Our conclusion is that RF-EMF should be regarded as a human carcinogen. The IARC classification should be updated to at least Group 2A, a probable human carcinogen. Current guidelines for exposure need to be urgently revised. The WHO Monograph draft on this issue is based on selective inclusion of studies and wrong assessment of the evidence of increased risk. Thus the Danish cohort study on mobile phone users and the Swedish Cancer Register data cannot be used as evidence of no increased risk. It is important that the public and decision makers are given correct information about the cancer risk so that they can make decisions based on correct data and take precautions. Otherwise there is an obvious risk of forthcoming increasing impairment of human health and increasing numbers of cancer in the population. We anticipate correction of the Monograph and your reply to this letter no later than 15 September, 2015. If you so wish our research group may of course give a presentation at WHO on this topic.
Yours sincerely,
Lennart Hardell, MD, PhD
Department of Oncology
University Hospital
SE-701 85 Örebro
Sweden
Michael Carlberg, MSc
Department of Oncology
University Hospital
SE-701 85 Örebro
Sweden